
Salah satu langkah penting dalam pengobatan kanker payudara adalah melakukan identifikasi jenis kanker payudara serta melakukan staging kanker payudara. Kanker payudara adalah salah satu kanker yang tersering dijumpai dan merupakan keganasan terbanyak yang ditemukan pada wanita. Akan tetapi, dengan teknik deteksi dini serta kemajuan terapi, saat ini tingkat mortalitas kanker payudara termasuk rendah. Hal ini dikarenakan kemampuan klinisi melakukan profiling jenis kanker payudara, sehingga pengobatan yang diberikan dapat lebih terarah dan hasil pengobatan menjadi lebih baik.
Secara umum tingkat survival atau kesintasan pada kanker payudara cukup baik dengan tingkat kesintasan 5 tahun adalah 90%. Namun, tingkat kesintasan ini menurun tajam sesuai staging kanker payudara yaitu 99% untuk kanker yang terlokalisir, 85% untuk kanker dengan penyebaran regional, dan hanya 27% untuk kanker dengan metastasis. Sayangnya, di negara Indonesia, masih banyak proporsi penderita yang datang pertama kali sudah stadium lanjut. Data di RS Kanker Dharmais tahun 2010 memperlihatkan pasien yang datang pada stadium III dan IV mencapai 63%.
Oleh sebab itu, walau sudah digalakan program awareness terhadap penyakit ini, namun tidak ada salahnya untuk melakukan penyebaran informasi mengenai kanker payudara seluas-luasnya. Salah satunya pada kesempatan kali ini, kita akan mencoba mengupas mengenai kanker payudara dimulai dari jenis serta bagaimana menentukan stadiumnya.
Daftar Isi
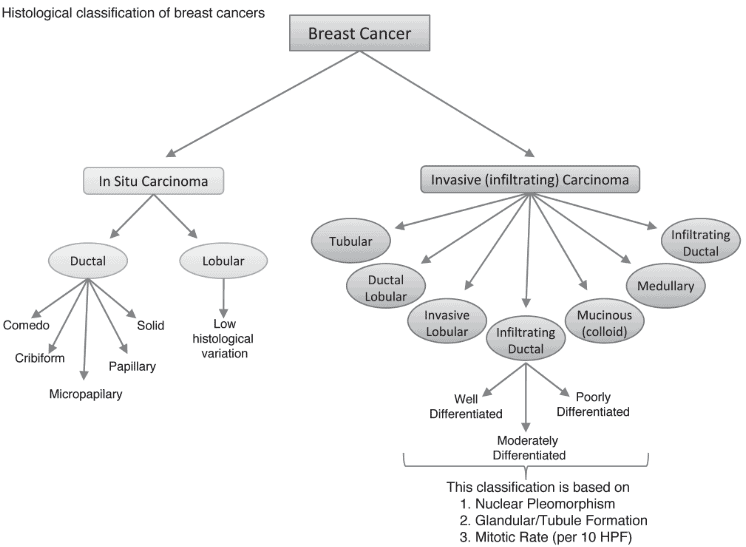
Klasifikasi Histologis Kanker Payudara
Secara genetis dan klinis, kanker payudara adalah penyakit yang heterogen. Terdapat berbagai jenis histopatologi serta karakter gen yang bervariasi dari kasus ke kasus. Skema pembagian dilakukan sesuai dengan prognosis dan terapi yang sesuai untuk setiap kelompok. Selain itu, saat ini juga berkembang klasifikasi yang memasukan karakter molekuler untuk setiap kasus kanker payudara
Pada stadium awal, sulit untuk membedakan lesi payudara apakah termasuk hiperplasia (tipikal dan atipikal), karsinoma in situ, atau kanker invasif. Oleh sebab itu, untuk lesi payudara biasanya langsung dibagi dua yaitu karsinoma insitu dan ivasif/infiltratif. Kemudian kedua kelompok ini terbagi lagi sesuai dengan bagan di bawah ini:
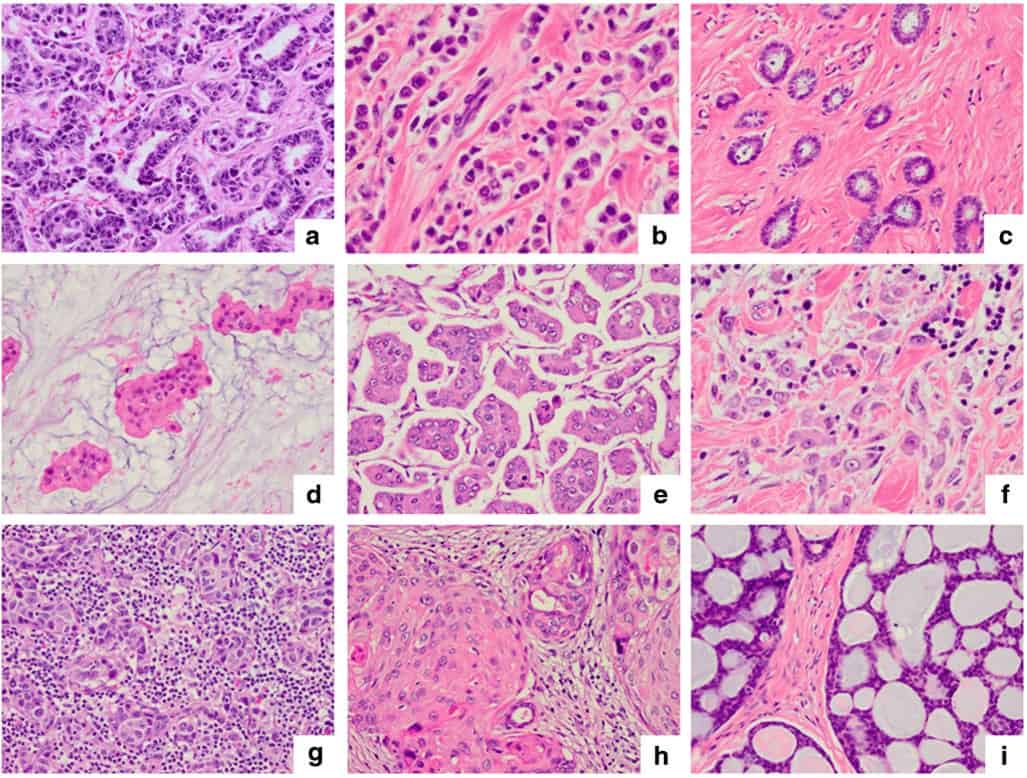
Adapun untuk gambaran histopatologi dari kanker payudara adalah sebagai berikut:
Karakteristik Molekuler Kanker Payudara
Pengenalan karakter molekuler terhadap kanker payudara sudah dilakukan sejak tahun 1950-an. Dimulai dengan identifikasi adanya reseptor estrogen (ER) yang kemudian diikuti pemanfaatannya untuk terapi hormonal pada kanker payudara. Selain untuk keperluan terapi, informasi adanya ER ini juga memberi petunjuk prognosis untuk rekurensi dan kesintasan.
ER ternyata bekerja kompleks dengan mempengaruhi oestrogen responsive elements di area promotor dari gen yang kemudian memodulasi dari proses transkripsi. Terapi hormonal berfungsi memblok ER dari hormon estrogen alami (tamoxifen) dan dengan menghambat produksi estrogen tubuh (inhibitor aromatase). ER juga dipengaruhi oleh faktor tumbuh lain seperti HER2 (melalui src atau MAPK) dan juga kompleks cyclin/CDK yang memodulasi melalui proses aktivitas kinase.
Reseptor progesteeron (PR) diregulasi oleh estrogen sehingga ekspresinya menggambarkan fungsi jalur sinyal ER yang intak. Ada kalanya tumor mengekspresikan ER namun tidak PR (ER+/PR-). Pada keadaan ini, terjadi kelainan atau mutasi pada jalur sinyal estrogen sehingga terapi hormonal kurang efektif pada keadaan ini.
Molekul lain yang ditemukan berpengaruh pada prognosis adalah HER2. Ekspresi berlebihan HER2 adalah indikator prognostik buruk dan juga petanda respon terhadap terapi dengan antibodi anti-HEr (trastuzumab, Herceptin). HER2 positif tampak pada 13-20% kanker payudara invasif dimana setengahnya tidak ada ekskpresi reseptor hormon (ER-/PR-). Pengaruh HER2 tehadap prognostik juga lebih terlihat pada kasus dengan sebaran KGB positif dibandingkan kasus tanpa sebaran KGB.
Kelompok lain adalah kasus dimana tidak terdapat ekspresi ER, PR, maupun HER2. Tumor tersebut disebut triple negative. Kasus tersebut memiliki morfologi dan perjalanan penyakit. Salah satu jenis dari kanker payudara triple negative ini jenis basal yang memiliki ekspresi tinggi dari sitokeratin bermolekul berat tinggi seperti CCK5/6 dan CK14 yang dalam jaringan normal juga diekspresikan oleh kompartemen sel basa/mioepitelial. Sel ini juga turut mengekspresikan EGFR (epithelial growth factor receptor). Kasus kanker sel basal payudara ini memiliki prognosis yang buruk dan tidak ada terapi target khusus yang bermanfaat. Termasuk ke dalam tipe basal ini adalah karsinoma dengan ciri meduler dan kanker payudara yang berhubungan dengan gen BRCA-1.
Petanda Molekuler Lainnya
Petanda molekul lain yang diperiksa pada kasus kanker payudara adalah Ki-67. Ki-67 adalah protein inti sel non histon yang menjadi petanda proliferasi atau pembelahan sel. Kepositifan dari Ki-67 bergantung pada kesintasan penderita yang lebih pendek. Namun, pemeriksaan rutin Ki-67 dibatasi oleh kurangnya standarisasi dan konsensus protokol penilaian sehingga interpretasinya bisa berbeda-beda. Di Indonesia sendiri, berdasarkan pengalaman saya, baik ER/PR, HER2, maupun Ki67 sudah biasa diperiksakan pada kasus kanker payudara.
Klasifikasi Molekuler Kanker Payudara
Berdasarkan pemeriksaan molekuler di atas, saat ini selain stadium, terdapat penggolongan kasus kanker payudara berdasarkan petanda molekuler. Adapun klasifikasi tersebut adalah seperti tabel di bawah ini:
| Tipe berdasarkan karakteristik molekuler | Tipe histologis | Grade histologis | Status ER oleh IHK | Status HER2 oleh IHK/ISH | Ki67 oleh IHK | Ciri molekuler khusus | Asosiasi integrated cluster yang predominan |
|---|---|---|---|---|---|---|---|
| Luminal A | IC-NST, classic lobular, tubular, cribriform, mucinous, neuroendocrine | 1–2 | 1–2 ER+ | HER2− | Low | PIK3CA mutations, MAP3KI mutations, ESR1 high expression, XBP1 high expression, GATA3 mutations, FOXA1 mutations, quiet genomes; gain of1q, 8q, loss of8p, 16q | Int cluster 2, Int cluster 3, Int cluster 4, Int cluster 7, Int cluster 8 |
| Luminal B | IC-NST, micropapillary | 2–3 | ER+/- | HER2-/+ | High | TP53 mutations, PIK3CA mutations, Cyclin D1 amplification, MDM2 amplification, ATM loss, enhanced genomic instability, focal amplifications (e.g. 8p12, 11q13) | Int cluster 1, Int cluster 2, Int cluster 6, Int cluster 9 |
| HER2 | IC-NST, apocrine, pleomorphic lobular | 2–3 | ER+/- | HER2+ | High | HER2 amplification, TP53 mutations, PIK3CA mutations, FGFR4 high expression, high expression, APOBEC mutations, Cyclin D1 amplification, high genomic instability | Int cluster 5 |
| Basal-like | IC-NST, medullary, metaplastic, adenoid cystic, secretory | 3 | ER− | HER2− | High | TP53 mutations, RB1 loss, BRCA1 loss, high expression ofDNA repair proteins, FOXM1 activation, high genomic instability, focal amplifications (e.g., 8q24) | Int cluster 4, Int cluster 10 |
| + positif, − negatif, +/−mostly positive, −/+mostly negative, ER oestrogen receptor, HER2 human epidermal growth factor receptor 2, IC-NST invasive carcinoma no special type, IHK imunohistokimia, ISH in situ hybridisation | |||||||
Staging Kanker Payudara
Staging dilakukan dengan sistem TNM mengikuti pola atau patokan seperti tabel di bawah ini:
| Tumor Primer | |
|---|---|
| TX | Primary tumour cannot be assessed |
| T0 | No evidence ofprimary tumour |
| Tis | Carcinoma in situ |
| Tis (DCIS) | Ductal carcinoma in situ |
| Tis (LCIS) | Lobular carcinoma in situ |
| Tis (Paget’s) | Paget’s disease (Paget disease) of the nipple NOT associated with invasive carcinoma and/or carcinoma in situ (DCIS and/or LCIS) in the underlying breast parenchyma. Carcinomas in the breast parenchyma associated with Paget’s disease are categorised based on the size and characteristics of the parenchymal disease, although the presence ofPaget’s disease should still be noted. |
| T1 | Tumour ≤20 mm in greatest dimension |
| T1mi | Tumour ≤1 mm in greatest dimension |
| T1a | Tumour >1 mm but ≤5 mm in greatest dimension |
| T1b | Tumour >5 mm but ≤10 mm in greatest dimension |
| T1c | Tumour >10 mm but ≤20 mm in greatest dimension |
| T2 | Tumour >20 mm but ≤50 mm in greatest dimension |
| T3 | Tumour >50 mm in greatest dimension |
| T4 | Tumour ofany size with direct extension to the chest wall and/or to the skin (ulceration or skin nodules)e |
| T4a | Extension to the chest wall, not including only pectoralis muscle adherence/invasion |
| T4b | Ulceration and/or ipsilateral satellite nodules and/or oedema (including peau d’orange) of the skin, which do not meet the criteria for inflammatory carcinoma |
| T4c | Both T4a and T4b |
| T4d | Inflammatory carcinoma |
| Regional lymph nodes (N) Clinical (cN) | |
| NX | Regional lymph nodes cannot be assessed (e.g. previously removed) |
| N0 | No regional lymph node metastases |
| N1 | Metastases to movable ipsilateral level I, II axillary lymph node(s) |
| N2 | Metastases in ipsilateral level I, II axillary lymph nodes that are clinically fixed or matted; or in clinically detectedk ipsilateral internal mammary nodes in the absence of clinically evident axillary lymph node metastases |
| N2a | Metastases in ipsilateral level I, II axillary lymph nodes fixed to one another (matted) or to other structures |
| N2b | Metastases only in clinically detectedk ipsilateral internal mammary nodes and in the absence of clinically evident level I, II axillary lymph node metastases |
| N3 | Metastases in ipsilateral infraclavicular (level III axillary) lymph node(s) with or without level I, II axillary lymph node involvement; or in clinically detectedk ipsilateral internal mammary lymph node(s) with clinically evident level I, II axillary lymph node metastases; or metastases in ipsilateral supraclavicular lymph node(s) with or without axillary or internal mammary lymph node involvement |
| N3a | Metastases in ipsilateral infraclavicular lymph node(s) |
| N3b | Metastases in ipsilateral internal mammary lymph node(s) and axillary lymph node(s) |
| N3c | Metastases in ipsilateral supraclavicular lymph node(s) |
| Regional lymph nodes (N) Pathological (pN | |
| pNX | Regional lymph nodes cannot be assessed (e.g. previously removed or not removed for pathological study) |
| pN0 | No regional lymph node metastasis identified histologically |
| pN0(i−) | No regional lymph node metastases histologically, negative immunohistochemistry (IHC) |
| pN0(i+) | Malignant cells in regional lymph node(s) not >0.2 mm [detected by haematoxylin and eosin (H&E) staining or IHC including isolated tumour cell clusters (ITCs)] |
| pN0(mol−) | No regional lymph node metastases histologically, negative molecular findings (RT-PCR) |
| pN0(mol+) | Positive molecular findings (RT-PCR), but no regional lymph node metastases detected by histology or IHC |
| pN1 | Micrometastases; or metastases in one to three axillary lymph nodes; and/or in internal mammary nodes with metastases detected by SLNB but not clinically detectedl |
| pN1mi | Micrometastases (>0.2 mm and/or >200 cells, but none >2.0 mm) |
| pN1a | Metastases in one to three axillary lymph nodes, at least one metastasis >2.0 mm |
| pN1b | Metastases in internal mammary nodes with micrometastases or macrometastases detected by SLNB but not clinically detectedl |
| pN1c | Metastases in one to three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by SLNB but not clinically detectedl |
| pN2 | Metastases in four to nine axillary lymph nodes; or in clinically detectedk internal mammary lymph nodes in the absence of axillary lymph node metastases |
| pN2a | Metastases in four to nine axillary lymph nodes (at least one tumour deposit >2.0 mm) |
| pN2b | Metastases in clinically detected internal mammary lymph nodes in the absence of axillary lymph node metastases |
| pN3 | Metastases in ≥10 axillary lymph nodes; or in infraclavicular (level III axillary) lymph nodes; or in clinically detectedk ipsilateral internal mammary lymph nodes in the presence ofone or more positive level I, II axillary lymph nodes; or in more than three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by SLNB but not clinically detectedl; or in ipsilateral supraclavicular lymph nodes |
| pN3a | Metastases in ≥10 axillary lymph nodes (at least one tumour deposit >2.0 mm); or metastases to the infraclavicular (level III axillary lymph) nodes |
| pN3b | Metastases in clinically detected ipsilateral internal mammary lymph nodes in the presence ofone or more positive axillary lymph nodes; or in more than three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by SLNB but not clinically detectedl |
| pN3c | Metastases in ipsilateral supraclavicular lymph nodes |
| Distant metastasis (M) M0 | |
| M0 | No clinical or radiographic evidence of distant metastases |
| cM0(i+) | No clinical or radiographic evidence of distant metastases, but deposits ofmolecularly or microscopically detected tumour cells in circulating blood, bone marrow or other non-regional nodal tissue that are not >0.2 mm in a patient without symptoms or signs of metastases |
| M1 | Distant detectable metastases as determined by classic clinical and radiographic means and/or histologically proven >0.2 mm |
| Staging anatomik | ||
|---|---|---|
| Stage 0 | ||
| Tis | N0 | M0 |
| Stage IA | ||
| T1 | N0 | M0 |
| Stage IB | ||
| T0 | N1mi | M0 |
| T1 | N1mi | M0 |
| Stage IIA | ||
| T0 | N1 | M0 |
| T1 | N1 | M0 |
| T2 | N0 | M0 |
| Stage IIB | ||
| T2 | N1 | M0 |
| T3 | N0 | M0 |
| Stage IIIA | ||
| T0 | N2 | M0 |
| T1 | N2 | M0 |
| T2 | N2 | M0 |
| T3 | N1 | M0 |
| T3 | N2 | M0 |
| Stage IIIB | ||
| T4 | N0 | M0 |
| T4 | N1 | M0 |
| T4 | N2 | M0 |
| Stage IIIC | ||
| Any T | N3 | M0 |
| Stage IV | ||
| Any T | Any N | M1 |
Kesimpulan
Saat ini selain staging kanker payudara secara anatomik berupa sitem TNM dan klasifikasi histopatologi, dilakukan pula staging berdasarkan profil molekuler terhadap kanker payudara. Hal ini akan berpengaruh pada diperlukannya terapi hormonal dan terapi target. Selain itu, profil molekuler juga bermanfaat sebagai faktor prognostik bagi pasien. Untuk informasi mengenai diagnosis dapat disimak pada artikel: Manifestasi Klinis dan Diagnosis Kanker Payudara, sedangkan untuk terapi dapat dilihat di artikel: Tatalaksana Kanker Payudara Stadium Dini (Early-Stage Breast Cancer)
Sumber
- Malhotra GK, Zhao X, Band H, Band V. Histological, molecular and functional subtypes of breast cancers. Cancer Biol Ther. 2010;10(10):955–60.
- Ng CH, Pathy NB, Taib NA, Teh YC, Mun KS, Amiruddin A et al. Comparison of breast cancer in Indonesia and Malaysia – A clinico-pathological study between dharmais cancer centre Jakarta and university Malaya medical centre, Kuala Lumpur. Asian Pacific J Cancer Prev. 2011;12(11):2943–6.
- Provenzano E, Ulaner GA, Chin SF. Molecular Classification of Breast Cancer. PET Clin. 2018;13(3):325–38.
- Senkus E, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rutgers E, et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol. 2015 Sep;26 Suppl 5(March):v8-30.

Seorang dokter, saat ini sedang menjalani pendidikan dokter spesialis penyakit dalam FKUI. Peminat berbagai topik sejarah dan astronomi.