
Hipernatremia merupakan kondisi berlebihnya kadar natrium darah, yaitu lebih dari 145 mEq/L. Adapun hipernatremia berat di artikan kadar natrium plasma ≥156 mEq/L. Kondisi ini menandakan hilangnya jumlah air dalam tubuh dan apabila berat dan akut merupakan kondisi kegawatdaruratan. Pada kesempatan kali ini akan di bahas tatalaksana dari kondisi tersebut. Gambar thumbnail oleh Hanjörg Scherzer dari Pixabay.
Daftar Isi
Regulasi Natrium dan Air Dalam Tubuh
Natrium sangat erat hubungannya dengan air dalam tubuh. Dalam pengaturannya, keduanya sangat berkaitan. Umumnya kondisi gangguan kadar natrium darah berhubungan dengan penyakit yang mengganggu kadar total air di dalam tubuh.
Walaupun lebih jarang dibandingkan hiponatremia, namun hipernatremia menyebabkan kematian yang besar sampai 40-60%. Oleh sebab itu, hipernatremia juga perlu mendapat perhatian dan menjadi salah satu kondisi kegawatdaruatan.
Keseimbangan Air dalam Tubuh
Salah satu kunci dalam memahami hipernatremia adalah mengaitkannya dengan komposisi utama tubuh yaitu air. Secara umum, total body water (TBW) meliputi 60% berat badan laki-laki dan 50% pada perempuan. Kemudian TBW ini dibagi lagi menjadi komponen cairan ekstraseluler dan kompartemen intraseluler. Komponen cairan ekstraseluler ini termasuk plasma, cairan interstitial, cairan limfe, jaringan ikat, tulang, cairan di kavitas tubuh, dan jaringan lemak. Perhatikan bagan di bawah ini:

Dari bagan di atas, tampak bahwa natrium merupakan komponen elektrolit utama dari cairan tubuh. Keberadaan elektrolit ini kadarnya dijaga ketat agar kekentalan atau osmolalitas cairan terjaga. Hal ini untuk menjamin agar fungsi sel dapat bekerja dengan baik.
Hormon yang Mengatur Keseimbangan Air
Cara tubuh mengatur keseimbangan air adalah terutama merasakan osmolalitas cairan. Di dalam tubuh osmolalitas dijaga dalam rentang 280 — 295 mOsm/L. Adapun reseptor perasa osmolalitas ini berada di pusat osmoreseptor berupa jaringan saraf yaitu organum vasculosum dari lamina terminalis (OVLT).
Selain OVLT, saraf pusat juga dilengkapi dengan neuron osmoreseptif yang tersebar luas di otak. Neuron osmoreseptif dapat ditemukan seperti di organ subfornical dan nucleus tractur solitarii. Jaringan ini dapat memungkinkan otak berespon secara integratif dalam mengatur osmilalitas cairan agar tetap dalam rentang normal. Caranya adalah dengan mengeluarkan berbagai macam hormon.

Berikut ini adalah berapa hormon yang berkaitan dengan regulasi air dan mempengaruhi kadar natrium darah:
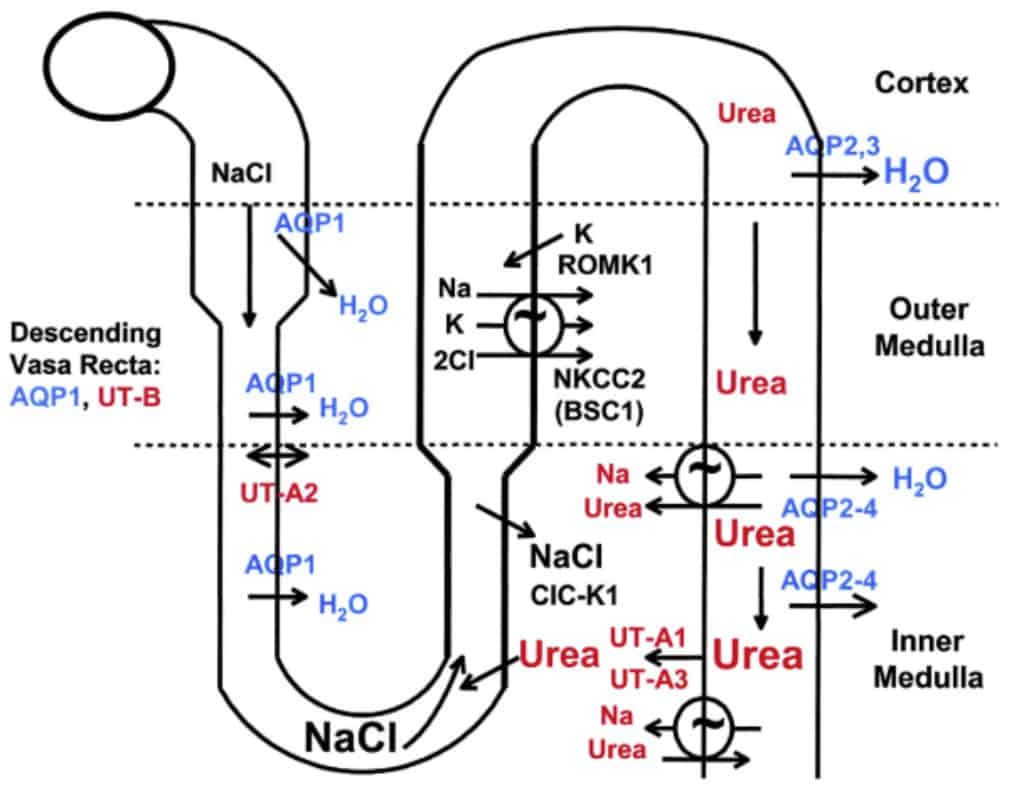
- Antidiuretic hormone (ADH). Hormon ini merupakan hormon utama yang mengatur konsenterasi atau kadar natrium. Pengeluaran ADH dirangsang oleh adanya kondisi hiperosmolaritas plasma, penurunan effective arterial volume (EAV), kerja angiotensin II. Kerja ADH menyebabkan insersi kanal aquaporin-2 di duktus kolektivus pada nefron ginjal. Hal ini menyebabkan reabsorpsi air sehingga meningkatkan osmolalitas urin. Osmolalitas urin (Uosm) tanpa ADH adalah 60 mOsm/L sedangkan dengan ADH maksimal 1200 mOsm/L.
- Aldosteon. Hormon ini mengatur jumlah total natrium dalam tubuh. Sekresi aldosteron terjadi ketika adanya hipovolemia (melalui renin dan angiotensin II), hiperkalemia (reabsorpsi isoosmotik dari natrium yang ditukar dengan kalium atau H+)
Patofisiologi Hipernatremia
Hipernatremia terjadi dalam kondisi adanya defisit air relatif terhadap jumlah natrium. Oleh sebab itu, semua pasien hipernatremia berstatus memiliki hipertonisitas.
Kondisi di atas terjadi akibat hilangnya cairan hipotonik bisa akibat dehidrasi atau masuknya infus cairan yang hipertonik. Selain itu dapat pula disebabkan oleh gangguan asupan air misalnya dalam kondisi intubasi, multiple sclerosis (MS), usia lanjut. Pada orang sehat, hipernatremia menimbulkan rasa haus yang kuat sehingga biasanya hipernatremia terjadi apabila pasien tidak dapat minum.
Etiologi atau Penyebab Hipernatremia
- Kehilangan air ekstrarenal (Uosm >700-800 mOsm/L)
- Saluran cerna: muntah, drainase nasogastrik (NGT), diare osmotik, fistula
- Insensible loss: demam, keringat saat aktivitas, ventilasi, luka bakar
- Kehilangan air di ginjal (Uosm <700-800 mOsm/L)
- Diuresis: osmotik (glukosa, manitol, urea), diuretik loop (misal furosemid)
- Diabetes insipidus, bisa bersifat sentral yaitu defisiensi ADH atau resisten terhadap ADH (nefrogenik)
- Sentral: penyakit hipotalamus atau gangguan pituitari posterior (kongetial, trauma/bedah, tumor, penyakit infiltratif/IgG4), dapat pula idiopatik, esefalopati hipoksik, keracunan etanol
- Nefrogenik: kongenital (mutasi reseptor V2 ADH, mutasi aquaporin-2), obat-obatan (liitum, amphotericin, demeclocycline, foscarnet, cidofovir), metabolik (hiperkalsemia, hipokalemia berat, malnutrisi protein, kelainan kongenital), penyakit tubulointerstitial (posobstruksi, fase pemulihan acute tubular necrosis/ATN, penyakit ginjal polikistik, sickle cell, Sjogren, amiloidosis), kehamilan (produksi vasopresinase dari plasenta)
- Lainnya (Uosm >700-800 mOsm/L)
- Overload natrium: cairan hipertonik (misalnya resusitasi dengan cairan bikarbonat/NaHCO3), kelebuhan mineralokortikoid
- Kejang: peningkatan osmol intraseluler menyebabkan pergeseran air ke dalam sel sehingga menyebabkan hipernatremia sementara di serum

Pendekatan Diagnosis Hipernatremia
Anamnesis bertujuan dalam menentukan penyebab hipernatremia. Riwayat trauma kepala dapat menjadi petunjuk ke arah diabetes insipidus sentral. Adapun riwayat penyakit psikiatrik dengan konsumsi obat lithium bisa menjadi kunci yang mengarah ke DI nefrogenik. Selain itu, hipernatremia yang terjadi dalam 48 jam digolongkan ke dalam hipernatremia akut sedangkan onset lebih dari 48 jam atau tidak diketahui dikategorikan ke dalam hipernatremia kronik.
Hipernatremia akut biasanya memberikan gejala yang lebih jelas dibandingkan kondisi kronik. Gejala tersebut dapat berupa letargi, kelemahan, iritabilitas, dan apabila berat dapat berupa kejang atau koma.
Dalam kondisi akut, otak dapat mengecil karena pergeseran air dari jaringan otak ke cairan plasma. Dalam kondisi ini, dapat menyebabkan volume otak mengecil dan bisa menyebabkan pecahnya pembuluh darah menyebabkan perdarahan subarachnoid dan/atau hematoma subdural. Namun, komplikasi perdarahan ini umumnya terjadi pada pasien bayi atau anak dibandingkan dewasa.
Hiperosmosis juga dapat menyebabkan kerusakan jaringan otot. Jika hal ini terjadi, disebut sebagai rhabdomiolisis hipernatremia. Dikarenakan pada kondisi kronik perubahan komposisi elektrolit lebih gradual, hal ini diikuti oleh perubahan kadar elektrolit yang gradual pula di kompartemen intraseluler sehingga gejala hipernatremia kronik menjadi kurang prominen dibandingkan kondisi akut.
Untuk menilai adanya hipernatremia serta penyebabnya, dilakukan pemeriksaan osmolalitas urin (Uosm), natrium urin (UNa), status volume cairan tubuh (tanda vital, ortostastik, tekanan vena jugular, turgor kulit, BUN, kreatinin). Kemudian untuk menentukan penyebab, dapat mengikuti alur di bawah ini:

Tatalaksana Koreksi Hipernatremia
Untuk tatalaksana hiponatremia berupa perbaiki akses terhadap air atau mencukupi kebutuhan air harian (≥1 L/hari atau biasanya 30-35 mL/kg/hari) serta mengganti defisit air beserta defisit volume cairan. Setelah volume cairan diperbaiki, langkah selanjutnya adalah menghitung defisit air dan jumlah cairan pengganti. Perhatikan persamaan di bawah ini:
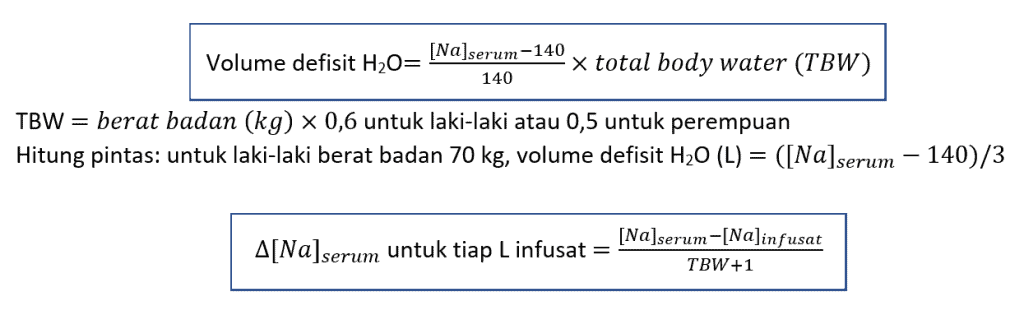
Misalkan, apabila kita akan memberikan cairan pengganti berupa dekstrosa 5% (D5W). Maka untuk tiap liter D5W yang kita berikan pada pria dengan berat 70 kg dan natrium tubuh 160 mEq/L akan menurunkan kadar natrium sekitar 3,7 mEq (D5W tidak mengandung natrium).
Perlu diingat bahwa penutunan natrium serum tidak boleh terlalu cepat, maksimal 0,5 mEq/L per jam atau 12 mEq/L per hari dan direkomendasikan hanya 10 mEq/L per hari. Jika terlalu cepat dapat menimbulkan edema otak. Misal, pada lelaki dengan berat 70 kg, pemberian air murni 125 mL per jam akan menurunkan kadarn natrium 0,5 mEq/L per jam. Sehingga pemberian air untuk pasien tersebut adalah maksimal 125 mL per jam.
Adapun target kadar natrium yang akan dicapai adalah 145 mEq/L. Adapun cairan infusat pengganti yang diberikan bermacam-macam. Bisa berupa D5W atau D5 ½ NS (natrium 77 mEq/L) atau D5 ¼ NS (natrium 38 mEq/L). Untuk D5 ½ NS dapat memberikan volume air bebas sekitar 500 mL per liter infusat sedangkan D5 ¼ NS 750 mL air bebas per liter infusat. Selain dalam bentuk infus, kedua cairan ini juga dapat diminum atau via NGT.
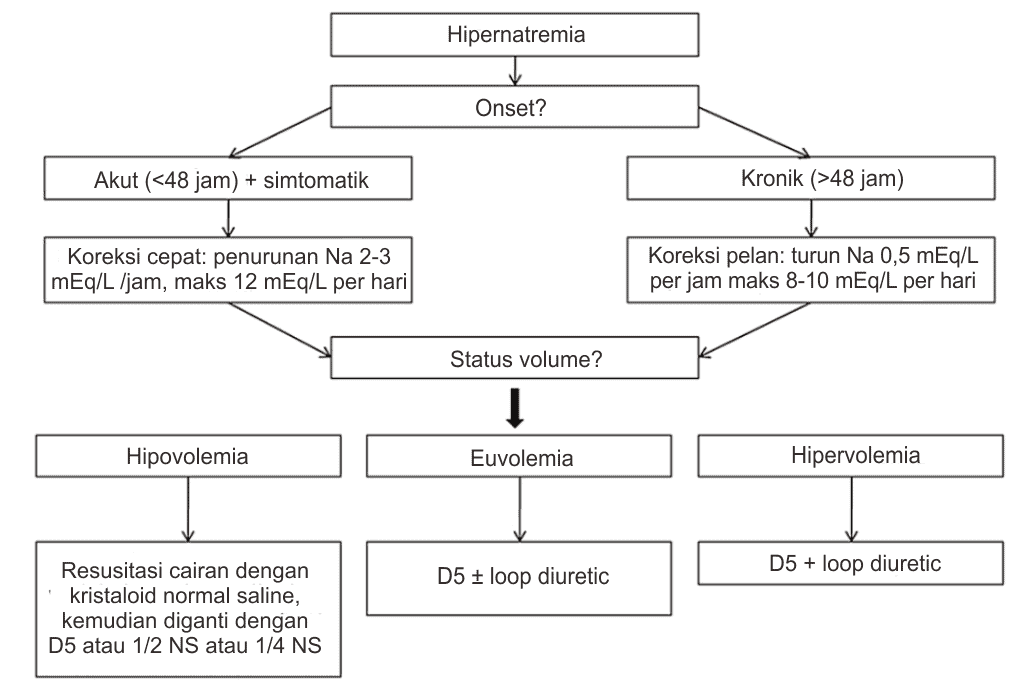
Untuk memudahkan perhitungan, kita dapat menggunakan kalkulator medis koreksi hipernatremia di tautan ini. Adapun untuk pengambilan keputusan, dapat mengikuti alur tatalaksana di bawah ini:
Tatalaksana Khusus Hipernatremia
Adapun jika penyebab hipernatremia akibat diabetes insipidus, jika penyebabnya sentral maka dapat diberikan desmopressin (dDAVP). Apabila penyebab DI nefrogenik, bila memungkinkan atasi penyebabnya, lakukan restriksi asupan garam plus thiazide. Hal ini akan menyebabkan deplesi volume ringan sehingga menurunkan keluaran natrium oleh ginjal. Pada kehamilan yang menyebabkan DI, dapat diberikan dDAVP.
Kesimpulan
Natrium sangat erat hubungannya dengan air. Kondisi hipernatremia pada dasarnya disebabkan oleh berkurangnya aasupan air yang menyebabkan dehidrasi atau kehilangan air yang banyak. Dalam kondisi normal, hipernatremia jarang terjadi karena kondisi ini merupakan rangsang haus yang sangat kuat. Dalam kondisi tidak adanya akses air baik ketiadaan sumber air atau kondisi medis tertentu, hipernatremia dapat dengan mudah terjadi.
Referensi
- Adrogué HJ, Madias NE. Hypernatremia. N Engl J Med. 2000 May 18;342(20):1493–9.
- Guillaumin J, DiBartola SP. A Quick Reference on Hypernatremia. Vet Clin North Am – Small Anim Pract. 2017;47(2):209–12.
- Lindner G, Funk GC. Hypernatremia in critically ill patients. J Crit Care. 2013;28(2):216.e11-216.e20.
- Muhsin SA, Mount DB. Diagnosis and treatment of hypernatremia. Best Pract Res Clin Endocrinol Metab. 2016;30(2):189–203.
- Sabatine MS, editor. Pocket medicine. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2014.

Seorang dokter, saat ini sedang menjalani pendidikan dokter spesialis penyakit dalam FKUI. Peminat berbagai topik sejarah dan astronomi.